
Most of us are never warned about it. You get a prescription, you take it as directed, and you trust that the people writing it have thought through the trade-offs. For the most part, they have. But there is one trade-off that rarely makes it into the conversation — the quiet way some long-term medications can drain the body of the very nutrients it needs to feel well. I see it in my practice constantly, and almost no one has been told to watch for it.
This is personal for me. When I was diagnosed with rheumatoid arthritis, I was started on several medications right away. What no one mentioned was how those drugs might deplete nutrients my body depended on. It wasn’t until I went deep into functional medicine that I understood the gap — not just in my own care, but in the care of so many patients who come to me tired, foggy, and aching, convinced that something is wrong with them when part of the story is sitting in their medicine cabinet.
The numbers most people never hear
Medication use is common, and it climbs with age. In any given month, roughly 46% of Americans use at least one prescription drug, and about a quarter use three or more — and among older adults, taking four or five daily medications is routine (CDC/NHANES). Yet only a small fraction of those patients are ever counseled about the nutrient cost of long-term use.
Here’s why that matters. The symptoms of a slow nutrient deficiency — fatigue, muscle weakness, brain fog, mood changes, a heart that flutters — look almost identical to “just getting older,” or to a brand-new health problem. So they often get treated with another prescription. That’s what I call the medication cascade: one drug quietly depletes a nutrient, the deficiency creates new symptoms, a new drug gets added for those symptoms, and the cycle keeps turning. The goal of this article isn’t to scare anyone off medications they need — it’s to help you close that loop.
I think of a woman in her early sixties who came to me feeling worse and worse despite doing everything right. She was on a stomach-acid medication, a statin, a water pill for blood pressure, and a diabetes drug. When we ran a thorough nutritional workup, she was genuinely shocked: she was low in magnesium, CoQ10, B vitamins, and potassium — and each one traced back to a medication she’d been told was helping her. None of those drugs were “wrong.” They just had a cost no one had accounted for.
Four common medications and what they quietly drain
Let me walk through the four I see most often. If you recognize yourself in any of these, it’s not a reason to stop — it’s a reason to have a smarter conversation with your prescriber.
1. Acid reducers (PPIs) and magnesium
Proton pump inhibitors — omeprazole, esomeprazole, the familiar purple-pill family — are some of the most-used drugs in the country, and they work by cutting stomach acid. The problem is that lowering acid also changes how well the gut absorbs magnesium. Back in 2011, the FDA issued a safety communication linking long-term PPI use (usually three months or more, often after about a year) to low blood magnesium (FDA).
Magnesium is one of those minerals that does a little of everything — it helps regulate blood pressure, fuels energy production in nearly every cell, calms inflammation, and steadies the heart’s rhythm. When it runs low for years, the effects are diffuse and easy to misread. I had a patient who’d taken a PPI daily for over fifteen years and arrived with stubborn fatigue and muscle cramps; his magnesium was severely depleted. Working with his doctor to find the lowest effective dose, and repleting magnesium thoughtfully, changed how he felt within weeks. Prolonged PPI users deserve periodic magnesium monitoring — full stop.
2. Statins and CoQ10
Statins lower cholesterol by blocking an enzyme in the cholesterol pathway — and that same pathway is where your body makes Coenzyme Q10, an antioxidant your cells use to generate energy. Studies show statins can lower circulating CoQ10 by somewhere in the range of 16% to 50% (the figure often quoted is around 40%).
I want to be precise here, because this is where a lot of internet advice goes off the rails. Most of the CoQ10 in your blood travels on LDL particles, so when a statin drops your LDL, your measured CoQ10 falls partly because the carrier dropped — not necessarily because your tissues are starved. And to be clear: CoQ10 supplements have not been shown to reliably fix statin-related muscle aches in trials. So I don’t treat CoQ10 as a magic antidote. What I do is take muscle symptoms and fatigue seriously, look at the whole picture, and consider CoQ10 as one supportive piece — especially in patients who are highly symptomatic. Statins protect a lot of hearts; the point is to keep their benefit while minimizing the collateral.
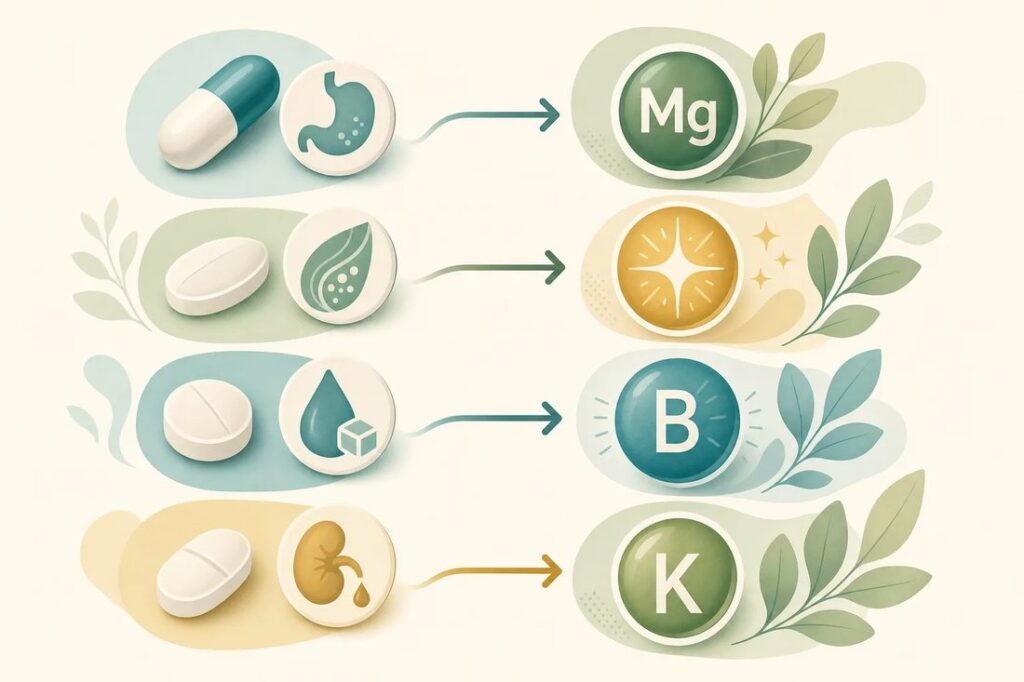
3. Metformin and vitamin B12
Metformin is a workhorse for type 2 diabetes, and a good one. But long-term use interferes with how the gut absorbs vitamin B12 — specifically by disrupting a calcium-dependent step in the lower small intestine, an effect that can often be eased with calcium. The popular claim that “30% of metformin users become B12 deficient” overstates it: in the better studies, roughly 4–8% of long-term users develop frank deficiency, with another 15–20% sitting in the low-to-borderline range (BMJ 2010).
That still matters, because B12 deficiency is sneaky. It can cause fatigue, tingling in the hands and feet, and cognitive changes — symptoms easily blamed on diabetes itself or on age. Low B12 can also nudge up homocysteine, a recognized cardiovascular risk marker. I’ll be honest about the science here: trials that lowered homocysteine didn’t reduce heart attacks, so it’s a flag, not a proven lever (HOPE-2, NEJM 2006). Still, anyone on metformin for years should have B12 checked periodically — it’s cheap to test and easy to fix.
4. Diuretics and your minerals
Water pills are prescribed for blood pressure and fluid retention, and by design they make you excrete more — including minerals you’d rather keep. Loop and thiazide diuretics reliably deplete potassium and magnesium, and they can increase urinary loss of zinc. Two nuances worth knowing: thiazides are actually the clearer driver of chronic magnesium loss, and high-dose loop diuretics (especially in heart-failure patients) have been linked to loss of thiamine, vitamin B1. The broader claims you’ll see online — that diuretics drain the whole B-complex, or wipe out CoQ10 — rest on much thinner evidence, so I keep my focus where the data are solid.
What to actually do about it
This is the part I want you to take away, because it’s empowering rather than frightening. Addressing medication-induced depletions is not about quitting drugs you need — it’s about keeping their benefit while closing the side door they leave open.
- Have the conversation. Ask your prescriber, plainly: “Could anything I’m taking long-term be depleting a nutrient, and should we monitor for it?” That single question changes the trajectory of care.
- Test beyond the basics. Standard panels miss a lot. Functional testing — red-blood-cell mineral levels, functional B-vitamin markers, CoQ10 — gives a truer picture of what’s happening inside the cell, not just floating in serum.
- Replete with quality, and care. Form and purity matter, and if you have any kidney involvement, supplement quality matters even more. This is exactly where guided IV and targeted nutrient support can help — delivered thoughtfully, not scattershot.
- Eat the cofactors. Whole foods bring nutrients alongside the cofactors that help you absorb them — leafy greens and seeds for magnesium, fish and eggs for B12, organ-rich and colorful diets for the rest. Supplements fill gaps; food builds the floor.
- Reassess periodically. Is every medication still needed at the same dose? Is there a version with a lighter nutritional footprint? These are fair questions to revisit with your doctor over time.

The bigger picture
The way I practice — combining the best of conventional and functional medicine — is really about asking the next question. Not just “what drug treats this symptom,” but “what is this symptom telling us, and is anything we’re already doing quietly contributing to it?” Nutrient depletion is one of the most overlooked answers to that question, and one of the most fixable.
Every person is different, with different root causes, and what helps one patient may not be right for you — results vary. And while I’m sharing this so you can advocate for yourself, I am not your doctor and I don’t know your specific situation. Please don’t change or stop any medication on your own; bring this to your prescriber and decide together.
If you’d like a more complete look at what might be depleting your energy — including comprehensive nutrient testing and personalized IV and supplement support — that’s exactly the kind of root-cause work we do at iVitality. You’re welcome to reach out and start the conversation.
Selected references: FDA Drug Safety Communication: Low magnesium levels can be associated with long-term use of PPIs (2011). · de Jager J, et al. Long-term treatment with metformin in type 2 diabetes and risk of vitamin B-12 deficiency. BMJ 2010;340:c2181 (PMID 20488910). · Qu H, et al. Effects of statins on coenzyme Q10: a meta-analysis. Eur J Med Res 2018;23:57 (PMID 30414615). · Lonn E, et al. Homocysteine lowering and cardiovascular events (HOPE-2). NEJM 2006;354:1567-1577 (PMID 16531613). · Kieboom BW, et al. Thiazide diuretics and risk of hypomagnesemia. Pharmacoepidemiol Drug Saf 2018 (PMID 30095199).
This article is for educational purposes only and is not medical advice. Always consult your healthcare provider before changing, stopping, or adding any medication or supplement.
Frequently Asked Questions
Can common medications deplete nutrients?
Yes. Many widely used prescriptions quietly lower specific nutrients over time. For example, acid reducers (PPIs) can reduce magnesium and B12, and statins can lower CoQ10. It is a well-documented trade-off that is rarely discussed at the pharmacy.
Which medications cause nutrient depletion?
Common ones include PPIs and acid reducers (magnesium, B12), statins (CoQ10), metformin (B12), and diuretics (potassium and magnesium). The effect builds slowly, so it is easy to miss.
Should I take supplements with my medication?
Sometimes, but not blindly. The right approach is to identify which nutrients your specific medications affect and replace them under medical guidance, since timing and interactions matter. Talk to your provider before adding anything.